In fact, we’ve written posts on here a few times regarding different ways therapists are stuck (or refuse to change) the way they practice. Quite often because of not wanting to include research in their practice, or committing to the new narratives around pain science etc.
If we did change, it often feels like a daunting task where the things we have been doing for so long have to change, and in turn there is sometimes fear around how our patients would react when this change occurs.
In the past, I’ve often chalked this up to the methods we use, or techniques we love become part of our identity and thus we don’t want to change.
While I still believe this to be true, it can’t be the only reason.
While reading a book recently, it dawned on me there could be another reason, which most of us probably don’t even realize. Mainly because this occurs subconsciously, it happens routinely, is performed regularly, and most of the time just happens automatically.
What I’m referring to a simple word that most of us don’t realize we are doing with every patient who comes in to see us.
Habits!
Little Seeds Of Change
Quite often when teaching or discussing different concepts around manual therapy with other practitioners, inevitably the topic always comes up “how do I incorporate this in practice”?
I’d say this is especially true with Massage Therapists and discussing how to begin including movement and exercise into treatments (this is just my take on discussions I’ve had with therapists, not the general rule).
There is usually a concern where the patient comes in and just wants to get on the table and get their treatment going. Even to the point of looking at their watch in an attempt to make sure they get their full hour on the table.
This was also true as I started getting interested in pain science and while learning along the way had to change my narrative with patients. I was genuinely worried (also due to my lack of confidence) that patients would think I sounded like I was out to lunch and start seeing a different therapist.
Well, the reality is, when I started doing more of both, not one of my patients ever looked at me and refused to do a movement, or told me they thought I was out to lunch (they may have thought it but never said it to me), and they very well could have because I’m sure it sounded like I was vomiting all this new information at them.
However, there is a way to do this in a much better way than I did when I first started trying to incorporate these things into my practice.
When we are trying to create change with a patient it’s usually about planting little seeds of information and playing the long game. It’s not always about making huge, grand changes all in one session. It’s about incorporating small changes over a longer period.
Perhaps it’s making one small change in an activity of daily living until eventually several changes are made and your patient adapts to a new routine or exercise until it becomes a habit.
So, if this approach can and does work for our patients, what if we took the same approach with our practice?
Changing Our Habits
In his book “Atomic Habits” James Clear breaks down how to build good habits and break bad ones.
One of the things I found really interesting was a quote from the book talking about habit change, I couldn’t help but relate it to how so often our techniques become part of our identity in our practice:
“The real reason habits stick is that it becomes part of your identity, improvements are only temporary until they become part of who you are”
“When you have repeated a story to yourself for years, it is easy to slide into these mental grooves and accept them as a fact. In time, you begin to resist certain actions because “that’s not who I am”. There is internal pressure to maintain your self image and behave in a way that is consistent with your beliefs. You find whatever you can to avoid contradicting yourself”
Just about everything we do in our clinic is a habit without even realizing it.
The way we greet a patient when they come in, the way we sit in our clinic room with them when they first arrive, the way our hands make initial contact with them when they’re on our table…all habits. We’re probably more likely to call it a routine, but these are all habits we’ve created, which is also part of the reason you’re successful.
Your patients REALLY like this routine.
And the thing is, so do we! It’s comfortable and familiar, which makes change all that much harder.
However, if we truly want to grow in our practice, it’s a matter of us deciding we will change, not making the patient change (although this will happen gradually).
This can also be daunting because it can feel like we’ll get left behind (making it all that much easier to stay in our groove), which is overwhelming, I mean, it takes 17 years before research is actually implemented in most medical practices, so it’s not like we’re going to get left behind by attempting to change what we do in our practice.
In this book, James talks about how to create new habits by doing something called “habit stacking”. To do this you identify a current habit you already do each day and then stack your new behaviour on top of the current one. As you begin to master the structure of doing this, you create larger change by incorporating more of these small changes until these new habits are formed.
Could we just start by asking one new question during our intake and do it with each patient one day, then the next, until it becomes part of our normal conversation with a patient? Once this becomes our new normal, we could include one graded exposure movement before each treatment? When this becomes part of the routine, start to incorporate movement into a treatment, then homecare, etc. Even if all we do is just change by a small fraction each day or week, this can have a profound change in our practice and our patients over the long term. As this adds up you can have some breakthrough moments that not only make you a better therapist but can enhance your career. And the best part is, while you gradually make this change, your patients will change with you without them realizing it. These changes will become an expected part of your treatment and hopefully, they won’t be checking their watch at the start of the treatment.
If you’re curious or want to know more about habit change and how it can help you and your patients, I highly recommend “Atomic Habits” which you can get HERE.
https://themtdc.com/wp-content/uploads/Massage-Therapist-Habits.jpg6871037Jamie Johnstonhttp://themtdc.com/wp-content/uploads/logo.svgJamie Johnston2020-07-28 07:55:232026-04-22 20:31:18How Changing Our Habits Can Change Our Practice
This is the first in the series of a few mini/microblogs of about 500 words (famous last words) and in this first one I wanted to kick off by talking about making movement and exercise meaningful.
This is a term that is being bandied about more and more in rehab but still has the feel of a buzzword rather than something well defined.
So what the hell does it mean……..
Firstly lets separate the idea of meaningful from what many describe as ‘functional’. Meaningful exercise does not have to look or recreate movements, mechanics, or even physical qualities that people may need.
Lets PLEASE not go down that road again. PLEASE.
Something being meaningful is much more about the WHY behind doing it or the meaning it holds (as the title suggests : )
Too often it’s the therapists why, but it really should be the PERSON doing it’s WHY! As therapists, we often have a bunch of why’s, ROM, strength, and other outcome measures that are often not really very well aligned with the patients WHY.
Put yourself in the other person’s boots – why am I actually doing this? And ultimately, by doing it, how can it help me? We pretty much do this calculation for a lot of things in life.
What makes this person tick when it comes to moving…..
Now it could be argued getting out of pain should be a big enough WHY. But when it comes to exercise, especially for rehab, we know that is not enough from the data around adherence (commitment is a much better word btw) and this also extends to adherence to drugs and general health advice.
So really we have to consider HOW to get to people’s WHY. Well, I think this really has to come from HOW we as HCPs interact with our patients. Without knowing what they want to achieve or their valued activities it is very hard to create a real relevance, MEANING, or as I like to call it a ‘finding a HOOK’.
Essentially any movement could be framed as being meaningful with the right explanation and the link to a motivating and meaningful goal. Learning more about sets and reps might not improve your outcomes!
Recent research has shown some very good effect sizes for using goal-setting interventions in back pain *HERE*
Here is real life an example from a course I gave last weekend in Melbourne. An attendee was discussing Jiu-Jitsu training. He said 50% of the reason he goes is for the social aspect. Firstly imagine the impact firstly of NOT going on life (more than just pain!), secondly the motivation to get BACK to going.
Rehab should tap into the meaning of that person’s life and what they gain from doing it, not just doing an exercise because someone told me to.
The problem has been one of therapeutic exercise finding an exercise to fix the problem, such as VMO firing for knee pain or core firing for back pain. Potentially we could call this targeting the muscle but missing the person. So we are now talking about movements not muscles, but how about talking people? Getting people moving perhaps needs a GOAL, a HOOK, a MEANING?
Maybe one of the benefits of working with a sporting or active population is that the WHY is often clear-cut, sometimes people can even be over motivated. The meaning is built into the process.
The challenge with persisting pain may be the motivation is not so clear cut, we need to dig a bit deeper as pain can narrow people’s focus and reduce the number of options they feel they have available to lead a full life. This is where ‘finding a hook’ can be really important I feel.
Meaningful movement tips
Listen and ‘find the hook’
Take time to explain WHY moving will help
Relate the explanations back to the ‘hook’
Spend time building confidence and positive movement experiences
Think person rather than exercise
P.s I was close – 650 words ; )
https://themtdc.com/wp-content/uploads/Massage-therapist-exercise-67.png6871037Ben Cormackhttp://themtdc.com/wp-content/uploads/logo.svgBen Cormack2020-07-20 20:51:112026-04-22 20:31:19Are You All About The Exercise Or The Person Doing It? Making Movement Meaningful
I understand the trend toward patient-empowerment, trying to build self-efficacy without risking dependency on the clinician. This has elevated the interventions of education and exercise over manual therapy in terms of best-practice recommendations for physical therapists.
As a long-term PT, I can understand this movement, but the trend comes at a price.
First off is the belief that manual therapy, viewed as a passive intervention, should be dosed sparingly as to not encourage dependency. In contrast, I contend that if manual therapy allows movement with less fear, pain, and caution, this, in itself, builds independence.
I do accept that more common view of PT is the exercise-based model, though I have HUGE issues with intellectual lazy PTs who blame weakness on pain. What I don’t and will not accept is an apparent lack of engagement on the part of my profession.
I have great respect for the time, patience, money, and emotional investment that a budding PT student makes to become a DPT, as it is not an easy path. But what are we building?
Recently I had dropped my car off for a service at a local repair facility. Rather than join the squad impatient chair-sitters, waiting for word of the bill in need of payment, I chose instead to take a long walk. This walk afforded me an opportunity to cruise through the nearby picturesque village, able to see the sights while getting my exercise. My walk took me past the village PT clinic…twice, once on my outbound journey, and again on my way back to the garage.
On my first pass, I was easily able to view a good handful of patients dutifully working out on at their respective stations, all seeming to be completely engaged in their tasks. But at the center of the facility, I viewed two individuals who I am assuming where the resident PTs. How did I know this?
Apparel, for one. They were the only ones NOT engaged.
Instead, they stood side by side, talking with each other, in the dreaded arms-crossed posture. Argh! OK, I thought, as I passed, maybe I caught them at a bad moment. Maybe it was a fluke. I’ll take a look on my way back, hoping that they would not be caught in such a compromising position.
The walk took me through the rest of the village and, with a bit of a divergence, along a roaring creek. Quite lovely. But as I again approached the PT clinic my suspicions rose and, sure enough, there they stood. Maybe they have moved and returned to the exact same spot to converse again…or maybe not. But there they stood, arms-crossed and conversing, while their patients dutifully went through their paces.
A PT may argue that those patients were engaged in self-helping behaviors, learning self-reliance, and building upon their own potential. Quite possibly.
But why did the PTs need to be standing there so unengaged? We can be more than arm crossers, we can be cheerleaders, encouragers, coaches, teachers, and, yes, occasionally, applying manual interventions. Self-reliance is key, but what has the PT profession become; a bunch of arm crossers? Manual therapy PT has its own skulls in the closet, but that’s not what this post is about. It’s about arm crossing.
My bias is toward using manual therapy as a primary intervention and evidence exists for this as a viable treatment strategy. I strongly discourage dependency of any sort and abhor it in other professionals. My work is set up to empower my patient to feel like they can move and with less fear. I teach them to self-treat, based on my examples, and make it a strong encouragement to engage in the movement of their choosing. I recognize that a good majority of patients seen for exercise-based PT improve, though those that don’t often come through my door.
As a profession, PT and other similar professions, the view of us by the public matters. Arm-crossing and spending a good amount of your time conversing with your peer instead of your patient is simply a lame way to spend medical dollars, not to mention a very expensive education.
Next time I make that walk, my hope is to see PTs engaged with their patient. They may not be touching, using manual therapy as I do, but I hope to see them spending time speaking to their patients, coaching and encouraging, aiding and correcting, prescribing, and adapting. I hope to see them doing the things our profession(s) are capable of and not resorting to the stereotypes that pockmark our profession.
BAN ARM-CROSSING
https://themtdc.com/wp-content/uploads/Untitled-design-66.png6381037Walt Fritzhttp://themtdc.com/wp-content/uploads/logo.svgWalt Fritz2020-06-09 07:19:402026-04-22 20:31:20Crossed Arm Syndrome
The Prone Press Up is one of the best ways to prevent and treat acute low back pain. Even if you get a massage, adjustment/manipulation, or other treatment in a clinic, you still need to maintain the improvement at home (unless you want to pay for a passive solution forever).
A patient is more likely to get better if they do a high dosage of repetitions throughout the day of whatever resets their system. If it hurts, they’re less likely to dose or to get to end range. Here are some of my favorite ways to make the prone press up pain-free or to eliminate the perception of tightness at end range
Any or all of these strategies should make the press up pain-free or as comfortable as possible so a high dosage should be easier to accomplish.
https://themtdc.com/wp-content/uploads/Press-Up-Massage-Therapy.png6871036Erson Religiosohttp://themtdc.com/wp-content/uploads/logo.svgErson Religioso2020-05-26 07:48:422026-04-22 20:30:04Level Up The Prone Press Up
Whether rehab exercises should be painful or not has become a recent topic of much discussion. As we have started to value the role of (optimal) loading in rehab, and that we can get patients back to moving and loading pretty early in the rehab process, we have also got to appreciate that this is unlikely to happen without experiencing any pain.
If you have any type of understanding about pain then the simple question of “should we use painful exercise?” suddenly might not look so simple!
Rather than a simple yes or no, there are a bunch of questions to be answered, such as how much pain is OK? Who may or may not benefit? And what is the best way to manage the process? Especially if all does not go to plan!
Research
From a data standpoint it would be great if we had have something that we can use to guide us here. Low and behold we do, and its open access.
This systematic review and meta analysis looked at 9 trials in which varying degrees of painful exercise were used. They found that painful exercise did NOT result in statistically worse outcomes across a short, medium or long term follow up. There was a small statistical benefit in the short-term for painful exercises as highlighted by the standardised mean difference of around 0.2 (SMD = effect size for a meta analysis). So from a research standpoint this is positive news.
One thing to note here from a clinical standpoint is, that using painful exercise is no GUARANTEE that it will have a positive effect for your patient. All statistical tests only give us the PROBABILITY of an effect, so the likelihood is that it will, but when we look at the confidence intervals (measure of variability) for the mean SMD for painful exercise, for the majority of the studies we can also see that they cross into a negative effect and in some of the studies quite substantially.
The variable effect of exercise on pain (although over a shorter time frame) was also shown by O Neill et al’s recent look at the acute effects of isometrics *Here*. Although, of course, isometric exercise and painful exercise is not the same thing, the point here is the highlighting of the variable effects from exercise. For patients with higher baseline pain isometrics actually increased their pain post exercise and this is the benefit of looking at individual responders within a study not just the group average. Those with lower pain at baseline seemed to receive more analgesia from isometric exercise.
BUT at the very least I think we can say that the likelihood is that it will not have detrimental effect. So as rehab can often be painful we can be reasonably confident but without seeing painful exercise as some sort of fire and forget panacea and also appreciate the individual nature of pain.
We could debate the mechanisms of HOW painful exercise might work from pain habituation to conditioned pain modulation and perceptual mechanisms but in essence we don’t really know at this point in time and this might be different or in different combinations for different people.
Benefits
The benefits can be both physical AND psychological.
Firstly, it allows patients to get in MORE exercise. If they are not being limited by pain (or pain contingent if we are being fancy :) then they can get a greater dosing than if they stopped due to it being painful. It is important to add though that we currently don’t know what optimal dosing is for exercise having an effect on pain!
Secondly, it sends the message that hurt does not equal harm. The problem can be painful and still settle down if managed in the right way. This may give people a new insight into their pain and how they can manage it.
Pain self-efficacy may also be built experientially, so using painful exercise as a tool might be an option to help do this.
Clinical Application
So it’s great to have some objective data on this subject, but as we know getting that into clinical application is not always straightforward.
Firstly don’t be afraid of some pain! The likelihood is that it won’t cause a worse outcome. But as we are dealing with thinking, feeling HUMANS, it is OF COURSE not as simple as this, but more on that later.
One of the issues with always looking to be pain free with exercise or continually treating pain, is what does that say ABOUT pain? On one hand we are telling people hurt does not mean harm but our actions might not be saying the same thing. If pain is OK, if it is normal then in the process of getting it better we might have to endure a little bit of it.
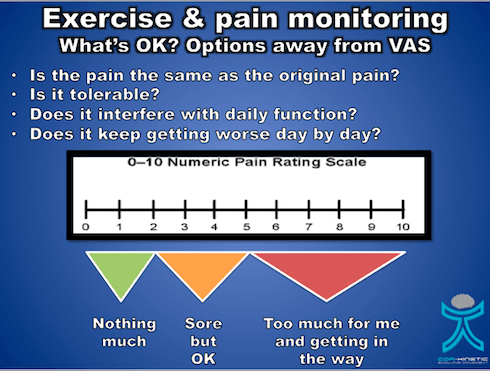
But how much is OK is a key question? Studies that have allowed painful exercise have ranged from not increasing baseline symptoms during or post exercise up to 5/10 on the VAS.
We know the limitations of the VAS as a REALLY subjective scale so perhaps we could introduce the idea of pain being tolerable or intolerable rather than a numerical score.
Now tolerable might be a bit sore but it does not really get in the way. Intolerable might be thought of as getting in the way of our daily activates, maybe having an effect on our sleep and generally making life a bit miserable. This is going to be different for different folk so hence why the concept of tolerable becomes important.
We would also like to know how the pain is settling down. So pain that is not really calming down after the exercise stimulus or keeps on getting progressively worse over a number of days as the exercises are performed is probably not a great idea. We would like to see a nice stimulus response with only slight increases above baseline (tolerable remember : ) that calms down gradually over 24-36 hours, quite similar to delayed onset muscle soreness (DOMS)
So on the issue of DOMS, it is important to identify if the increase in pain is actually the same as the original symptom. Post exercise soreness is quite normal but for those that are unaccustomed to exercise this might not be recognisable especially for a currently painful area. Defining what is pain and what is soreness might be a good sense making exercise for some patients. Although we don’t know that progressive overload is required with exercise in rehab, it probably ia a good idea, so having some sort of tolerable baseline for patients to progress or regress from is a great idea too. This is also might have an effect their self efficacy using exercise too which, of course, is a bonus.
Pain Is Not The Only Issue
Potentially the most problematic area with painful exercise, and one that is really under discussed, may be more about the psychological aspects that are associated with the pain and how they can affect the person. One of the best prognostic factors for recovery in a number of body areas appears to be pain self efficacy, *here* is a recent paper from Chester et al and also from Foster et al *here* Pain self efficacy, something I have written about before also *here*, is the ability to carry on normal functioning despite of pain. It is important to note that those with higher pain self efficacy also tend to adhere to exercise better.
So someone’s pain self efficacy is going to be a KEY factor in whether they are able to tolerate having pain and being able to carry on functioning which maybe a fundamental skill at the heart of painful exercise especially if it can take 24-36 hrs to settle.
Predicted outcome is another key prognostic factor and if someone believes that increased pain will result in a negative outcome then this could have a negative effect on the actual outcome.
Jack et al *here* found that the number one reason for poor adherence to exercise programs was that people did not want to make the problem worse. So painful exercise coupled with negative beliefs about pain, low pain self efficacy and a poor predicted outcome may not sit well together.
Firstly you could screen people for these factors if you feel they are required. We have tools such the Pain Self Efficacy Questionnaire (PSEQ) and the shorter version the PSEQ-2.
One caveat with using questionnaires, in my opinion : ), is it does allow us to get a score to assess confidence and resilience in managing pain but it perhaps does not tell us about things that are specific to our patients. So being able to weave this into a good subjective that teases these more personal parts of the narrative out is a must.
Also ASK about their expected outcome from the treatment and what would it mean to you if it was painful.
“Do you feel like this exercise will work for you?”
“Do you have any concerns about doing this exercise?”
It might be that someone tells you that they have tried exercises before and they did not work or that they feel it might make the issue worse, especially if it hurts.
It might also be important to discuss with ALL patients what their beliefs are around pain. These might be that pain indicates they are doing more damage to their bodies or they will not be able to work because they have pain or implications for future functioning. It can often be what the pain MEANS to the patient that is the real issue rather than just the sensation of the pain itself.
A key factor to remember is regardless of whether painful exercise is positive or no worse than non painful exercise, a negative belief may stop your patient from exercising
Education
One of the most powerful tools we have at our disposal is EDUCATION, I am not always a huge fan of this term as it can imply a teacher pupil relationship. But in order to provide effective education to people we first have to build rapport and then understand what they may need to know more about.
We can educate on a range of things from the effectiveness of exercise for many issues, that painful exercise is often not detrimental, that pain self efficacy is an important prognostic factor and what pain may actually mean and its relationship with physical damage. It may also be worth talking about the process and what to expect, and often that it is a process of trial and error to get the right level and desired response.
This has to start with understanding the patient, their history and belief structure.
Where You Start Is Not Where You Have To Finish
Do we have to jump straight into painful exercise? I don’t think so. It is not REQUIRED but it is also not harmful.
An important point to make is that for someone with very negative beliefs about pain, reduced pain self efficacy and poor beliefs about the outcome, challenging them right off the bat with painful exercise might not always be the best thing to do. As they build trust in you and confidence in their bodies then pushing into pain progressively might sometimes be a better route.
We know that giving people the option to avoid pain can actually maintain pain avoidance, so whilst not advocating avoidance behaviour confronting these things may take a little time, confidence and education, especially if the person has a lot of negative pain and avoidance based beliefs.
Those that persist in doing painful things that have NOT provide a therapeutic effect may benefit from non painful exercise for a while too. If you feel that pushing into pain has not given the desired response when looking at their history then a break or change in dosage could be just the ticket.
Those with higher levels of pain at baseline on average seem to have worse clinical outcomes so this might also lead me to reason that maintaining this level of pain through exercise might not always be a good idea.
There are no real hard and fast rules here only individuals and individual considerations.
What If It All Goes Wrong???
This is where self efficacy may come into its own. Empowering your patients to self manage maybe valuable in the exercise process.
As we hopefully have told the patient BEFORE they embark on an exercise program I can often be trial and error. Have we enabled our patients to adapt their exercise dosage if it goes a bit wrong? *Here*is a short piece on dosage in rehab
So do your patients know what to look out for in terms of symptoms?
Do they know how to adjust the dosage? This could be in exercise frequency, intensity and time, sets and reps (volume).
Are they able to contact you to ask questions? Do they know this?
I think these are all required aspects of pushing into pain.
A patient I saw last week had religiously persisted at pushing into his painful rehab exercises every 48hrs. He believed if he did what he was told he would get better (the trust!). But after 3 months there was not the desired outcome. In this case he was given no indication what to do if this happened, just blind faith on all sides that he would get better.
Key Points
Painful exercise DOES NOT produce worse outcomes from the research we have
Research does not guarantee your patients response to painful exercise
It is not just about the PAIN sensation! What does the pain mean and how does it affect behaviour such as exercise adherence?
Pain self efficacy and predicted outcome are important psychological measures and can be discussed and measured
Think about education around the exercise and the pain response
It does not need to start with painful exercise!
Empower your patients to self manage
https://themtdc.com/wp-content/uploads/Massage-Therapy-Painful-Rehab.png6871036Ben Cormackhttp://themtdc.com/wp-content/uploads/logo.svgBen Cormack2020-05-18 20:07:562026-04-22 20:30:05Painful Exercise In Rehab – Yes, No, Or A Lot To Think About
This is one of my favorite old school manual therapy techniques I learned while in Fellowship with the University of St. Augustine.
When my current techniques of tibial IR, lateral tibial glide, or other Functional Mobilizations I do in closed chain don’t work to improve knee flexion, I try this knee tilt.
It can be enhanced or made much more comfortable with an EDGE Mobility Band. Try this mobilization and let me know what your results are!
We may request cookies to be set on your device. We use cookies to let us know when you visit our websites, how you interact with us, to enrich your user experience, and to customize your relationship with our website.
Click on the different category headings to find out more. You can also change some of your preferences. Note that blocking some types of cookies may impact your experience on our websites and the services we are able to offer.
Essential Website Cookies
These cookies are strictly necessary to provide you with services available through our website and to use some of its features.
Because these cookies are strictly necessary to deliver the website, refusing them will have impact how our site functions. You always can block or delete cookies by changing your browser settings and force blocking all cookies on this website. But this will always prompt you to accept/refuse cookies when revisiting our site.
We fully respect if you want to refuse cookies but to avoid asking you again and again kindly allow us to store a cookie for that. You are free to opt out any time or opt in for other cookies to get a better experience. If you refuse cookies we will remove all set cookies in our domain.
We provide you with a list of stored cookies on your computer in our domain so you can check what we stored. Due to security reasons we are not able to show or modify cookies from other domains. You can check these in your browser security settings.
Other external services
We also use different external services like Google Webfonts, Google Maps, and external Video providers. Since these providers may collect personal data like your IP address we allow you to block them here. Please be aware that this might heavily reduce the functionality and appearance of our site. Changes will take effect once you reload the page.
Google Webfont Settings:
Google Map Settings:
Google reCaptcha Settings:
Vimeo and Youtube video embeds:
Privacy Policy
You can read about our cookies and privacy settings in detail on our Privacy Policy Page.