Should Massage Therapists Wade Into The Nutritional Arena?
Nutrition is a fascinating and important subject.
After sleep, diet is likely the most important factor affecting our health.
According to the most rigorous analysis of risk factors ever published—the Global Burden of Disease Study—the number one cause of death in the United States, and the number one cause of disability, is our diet.(1)
This is how important diet is.

Our collective knowledge in the area of nutrition continues to grow rapidly with thousands of studies published every year.
We know more about nutrition than at any other point in history, and yet paradoxically North Americans are at record overweight and obesity levels. And while these levels are finally slowing down, they have yet to actually level out or decline.(2)
I developed an intense interest in nutrition after watching the documentary Forks Over Knives in 2013.
This led to immediate and profound changes to my diet so that I could correct some personal health issues.
Since that time, I have found myself reading on the topic of nutrition almost daily. While this knowledge is extremely useful to me personally, offering nutritional advice is not within our scope of practice.
However, as you know, the topic can come up during an assessment or a treatment.
What can you say or do when this happens? This may depend on the scope of practice guidelines in your jurisdiction. Here is the scope of practice for massage therapists within the province of Ontario, Canada, where I work.
“The practice of Massage Therapy is the assessment of the soft tissue and joints of the body and the treatment and prevention of physical dysfunction and pain of the soft tissue and joints by manipulation to develop, maintain, rehabilitate or augment physical function, or relieve pain.” (Massage Therapy Act, 1991)
There is no mention of the words nutrition or diet, so one could safely say that this area therefore falls outside of our scope.
We can assess soft tissue dysfunction, but our treatment options are limited to ‘manipulation’. The only way that we could directly advise in nutrition is if we possess certifications in nutrition. In this case we have to take off our (figurative) massage therapy hat, and put on our nutrition hat.
While we cannot, and should not offer specific dietary advice, we can certainly inquire about our client’s dietary habits if they are experiencing delayed, or stalled healing.
For clients curious to learn more, we can suggest evidence-based resources, or we can refer to qualified professionals.
However, to be able to do this we need to have a basic understanding of nutrition ourselves. If there were two reasons for gaining extra knowledge in nutrition, I would list atherosclerosis and inflammation as two major factors.
We are all treating the effects of these conditions every day, and diet affects both of them.
Atherosclerosis
For body tissue to remain healthy, oxygen, nutrients, and cellular building blocks all need to be delivered to our soft tissue.
As well, cellular metabolites need to be removed from these tissues.
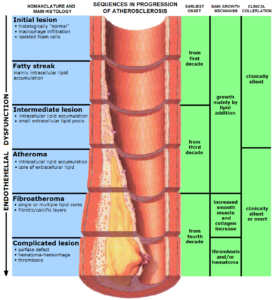
This role is performed by our circulatory and lymphatic systems. However, it might surprise you to learn that by age 10 nearly all children have fatty streaks in the arteries that deliver these nutrients to the body.(3)
These streaks are the first sign of atherosclerosis (the leading cause of death in the United States, and the second leading cause in Canada).
For people eating the standard North American diet, atherosclerotic plaques typically start forming in their 20s, and then become progressively worse with each successive decade.
The reason that nutrition is so important is that we now know, thanks to independent studies done by both Dean Ornish(4) and by Caldwell Esselstyn(5), that atherosclerosis is largely a diet-related disease.
Diet is so powerful that a healthful diet has been shown to actually reverse atherosclerosis.
Ornish et al. proved this using quantitative angiography on his test subjects. So, rather than accept that atherosclerosis as an inevitable consequence of aging, we now know that we do not need to see these sorts of degenerative changes happening in our (and our patients’) circulatory system.
To give you an idea of how profound these changes are, take a look at healthy vertebral arteries below (a), and then vertebral arteries clogged with atherosclerotic plaques (b).
It does not take a PhD in nutrition to realize that these blockages will result in radically altered nutrition to the soft tissue surrounding the spine.

http://www.ncbi.nlm.nih.gov/pubmed/19328027
In the coronary arteries, atherosclerosis can manifest as angina (or more seriously as coronary thrombosis), but these are not the only arteries affected.
In our extremities, atherosclerosis can manifest as numbness and tingling.
If blockage worsens, clients can experience intermittent claudication, an extremely debilitating condition.
Atherosclerosis has also been implicated in other conditions that we treat such as degenerative disk disease(6), disk herniation(7), sciatica(8), radiculopathy(9), and idiopathic back pain(10).
This should make all massage therapists stand up and pay attention to the role of diet as it relates to soft tissue dysfunction. If soft tissue is not receiving adequate blood flow, tissue health will suffer.
Inflammation
Atherosclerosis is actually an inflammatory disease of the arteries, but as you know, inflammation can occur anywhere in the body.
Many foods and dietary constituents have inflammatory effects on the body, and this sets the body up for a host of inflammatory conditions such as tendonitis, tenosynovitis, arthritis, plantar fasciitis, and other conditions that we treat on a daily basis.
Diet plays a key role in inflammation, either adding fuel to the fire, or helping to reduce inflammation.
Research into the field of the human gut bacteria is currently getting a lot of funding so there has been an abundance of research into this fascinating area, and it has become apparent that the gut is intimately involved in inflammation.
Dietary fibre is the primary food of our gut bacteria and fibre plays a key role in dampening inflammation(11).
This is only one example of how diet can promote or attenuate inflammation. Many foods have a pro-inflammatory effect, while others are anti-inflammatory.
I am sure that most of us have had the experience of chasing inflammation from one area of a client’s body to another. For example, a client might present with lateral epicondylitis. Then, before that issue is resolved, plantar fasciitis appears. Then, just when you get the previous issues resolved, idiopathic frozen shoulder mysteriously appears.
Once I gained an understanding of nutrition, puzzles like this were much easier to solve.
This is not to say that a client will necessarily change their diet once they learn its role in their health, but they do have a right to this information. Then they can make an informed decision, and the concept of informed choices is at the heart of health care and patient rights.
So, you can see how it would be beneficial for us to develop a basic understanding of nutrition as it relates to inflammation.
In Conclusion
For where I sit, I would say that there are likely more personal, rather than professional reasons for becoming more nutritionally literate.
The reason for this is due to our current scope of practice.
If you educate yourself on the topic of nutrition, you will learn a lot of valuable information that you (frustratingly) will not be able to directly incorporate into your daily practice.
However, having opened up the Pandora’s Box of nutrition, I would say personally that I never want to go back to a state of ignorance.
I got into the health field to better understand health and the human body, and understanding nutrition has give me for more power over my health than I could have ever imagined.
As a Massage Therapist, you are not required or expected to have a nutritional background. However, therapists in regulated provinces in Canada are well educated in physiology and pathology, so they possess the background information to appreciate understand the important role of nutrition in patient health. If you do take courses or educate yourself in this area, it will open new doors for you, but on the downside, you cannot offer direct nutritional advice as a Massage Therapist. However, with a proper nutritional knowledge base, you will know when either to refer to a nutritional professional, or where to direct your client to evidence-based nutrition resources.
I will leave the last word to Dr. Greger of NutritionFacts.org. Click on the link below to find out why you should care about this topic. Why You Should Care About Nutrition:
http://nutritionfacts.org/video/why-you-should-care-about-nutrition/
References:
- Murray CJ, Atkinson C, Bhalla K et al. The state of US health, 1990-2010: burden of disease, injuries, and risk factors. JAMA. 2013 Aug 14;310(6):591-608.
- http://stateofobesity.org/obesity-rates-trends-overview/
- J. P. Strong, H. C. McGill. The pediatric aspects of atherosclerosis. J Atheroscler Res 1969 9(3):251 – 265.
- Ornish D, Brown SE, Scherwitz LW, et al. Can lifestyle changes reverse coronary heart disease? The Lifestyle Heart Trial. Lancet. 1990 Jul 21;336(8708):129-33.
- Esselstyn. C.B., Gendy,G., Doyle, J. A way to reverse CAD? J Fam Pract. 2014 July;63(7):356-364
- L I Kauppila. Atherosclerosis and disc degeneration/low-back pain–a systematic review. Eur J Vasc Endovasc Surg. 2009 Jun;37(6):661-70.
- U G Longo, L Denaro, F Spiezia, F Forriol, N Maffulli, V Denaro. Symptomatic disc herniation and serum lipid levels. Eur Spine J. 2011 Oct;20(10):1658-62.
- P Leino-Arjas, L Kauppila, L Kaila-Kangas, R Shiri, S Heistaro, M Heliovaara. Serum lipids in relation to sciatica among Finns. Atherosclerosis. 2008 Mar;197(1):43-9. Epub 2007 Sep 7.
- P Leino-Arjas, L Kauppila, L Kaila-Kangas, R Shiri, S Heistaro, M Heliovaara. Serum lipids in relation to sciatica among Finns. Atherosclerosis. 2008 Mar;197(1):43-9. Epub 2007 Sep 7.
- L I Kauppila, R Mikkonen, P Mankinen, K Pelto-Vasenius, I Maenpaa. MR Aortography and Serum Cholesterol Levels in Patients With Long-Term Nonspecific Lower Back Pain. Spine (Phila Pa 1976). 2004 Oct 1;29(19):2147-52.
- Kuo SM The interplay between fiber and the intestinal microbiome in the inflammatory response. Adv Nutr. 2013 Jan 1;4(1):16-28.