Chain Of Command In Sports Massage
When I first started in the fire service, I didn’t fully understand why we had chiefs, captains and lieutenants, this thing we call “chain of command”.
All I knew was there were people telling me what to do and I’d better listen.
As I progressed it became more clear why this was necessary and how it applied to what we were doing.
I never gave it much thought outside of the fire service but have now come to understand how “chain of command” is applicable and necessary in sports and working with teams as a Massage Therapist.
While it can be a bit tough to understand (and some may find it insulting) there is a purpose and very good reason behind having chain of command in place. It is also important to understand how to work within it if you are going to be successful working with teams.
You may not always agree with how this type of organization works but if you want to work effectively and be part of the team, you have to work in accordance with the team principles.
Here’s why and how to do it.
Principles Behind This Organization Style
If you’re already working with teams you might be familiar with this, but if not it’s important to understand the structure.
Businesses, organizations and emergency services all operate under this kind of functional system in order to operate more efficiently and to work within it, you have to understand not only your role, but also the terminology behind it.
Here is some of the terminology, it may not be used extensively when working with a sport team, but the basics are the backbone of the way most organizations have things set up:
- Chain Of Command
- The formal line of authority, responsibility and communication.
- Unity Of Command
- A principle that each employee reports directly to one supervisor moving up the chain, ultimately all report to the main person in charge.
- Span Of Control
- The principle that establishes the maximum number of people or functions that any one supervisor can control, it’s typically three to seven but five is considered optimum.
- Division Of Labour
- This is the process of dividing larger jobs into small jobs to make them more manageable and efficient.
Below is how an organizational chart could look for a large team (obviously I picked hockey).
*This is just an example, not necessarily how any one team is set up.
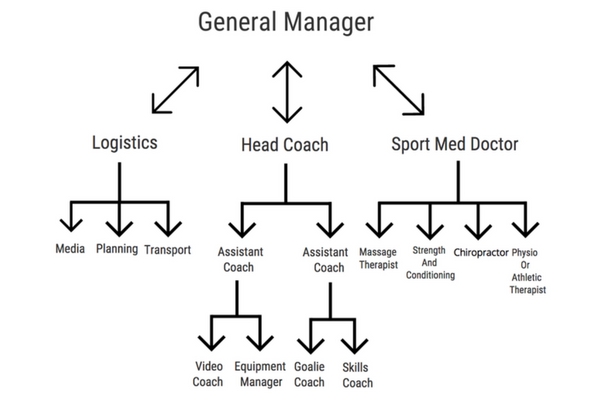
As you can see, the General Manager would ultimately be in charge with Logistics, Head Coach and Sport Med Doctor all reporting directly to him/her.
They would each then oversee their own group who would report to them.
In our case, the Sport Med Doctor would oversee the healthcare of the athletes with Massage, Strength, Chiro and AT all reporting directly to them, they would then convey the necessary information the the General Manager.
Remember, the above is just an example. It may be set up where the Massage Therapist reports to the Physio, who reports to the Doctor.
These lines of communication are essential in the function of any organization, since each person can only effectively manage five people (according to span of control).
Having things organized this way also gives the organization room to expand (or decrease) if necessary. For instance, the General Manager can add assistant GM’s as the organization expands giving them new branches of responsibilities and groups operating under them.
Understanding how you fit into these lines is essential, not only to your success, but to the teams success as well.
Know Your Role Jabroni!
Okay, so you’re not a jabroni, but it’s a good headline to get the point across.
If you’re selected to work in this kind of team environment, knowing your role is crucial.
The team probably even has a job description prepared for each person on the medical team, outlining each persons specific role. Not all the roles will be specifically medical.
Depending on your past relationship with a team or whether you’re brand new can define what your role will be, or how you can function within the role they define and the scope that is laid out for you.
Initially you may have a very minor role. The A.T, Physio or Sport Doctor may be the ones who do all of the assessment and refer athletes to you only when they deem necessary.
Don’t take this as a slight against you if this is how things start out!
The team may have things designed that way because of insurance concerns, or because of past experiences which are totally beyond your control. Don’t forget, there is a broad spectrum of massage therapy certifications out there in addition to the broad spectrum of experience these other healthcare professionals in working with Massage Therapists.
The job description given to you may have you assisting equipment managers, helping with video, filling water bottles, or just cleaning up the dressing room.
Again, it’s not a slight against you or the profession, it’s just a role the team needs filled, so they might get you to help out by filling that role.
Now, the rest is up to you.
Personalities play a massive role in team sports. When you’re starting out be happy to fill whatever role it is they have designated for you. Leave the ego at the door. As you start to work more regularly with the team, your role can expand, it’s all about building that relationship (where have I heard that before?). As the trust builds between you and the other healthcare professionals in the group, so will your role and what you can do. It’s all part of being a team, not all jobs on the team are going to revolve around you doing soft tissue work on athletes. Nor is all the work for the other healthcare professionals going to solely revolve around healthcare for the athletes, it’s about pulling together for the greater good of the team. Like it or not there is still a hierarchy, these other therapists have more education than we do and may assume that we report to them, even though the team chain of command doesn’t display that. Back to those personalities, while some people will bring their ego and put it on display, that usually gets weeded out. You may just have to change your approach in dealing with people for the greater good of the team. If someones ego is getting in the way, it may be something you have to work around temporarily, but trust me it will be temporary.