We published an article earlier this week about the therapeutic alliance. What we didn’t talk about in that article is how it is our responsibility to build and maintain that relationship. Fortunately, there are other therapists out there blogging and covering why this is important.
We preach regularly about evidence-based practice around here. This article lays out not only the importance of this, but also how to be reasonable about it when taking into account our clinical experience.
This past couple of months have been hard on everyone’s business. As a result, many of us could be experiencing some self-doubt regarding their progress and business success. This self-doubt can have major impacts on how we do things, but there are ways to curb this thinking and get back on track.
If you’ve been following this blog for any length of time, you know how strongly we feel about exercise. While the findings and studies are new and limited still, there is emerging evidence to show how important exercise is an effective way to manage stress during to local public health restrictions.
We have published many an article showing how to do graded exposure with patients. While this article is directed towards mental health professionals, the same arguments can be made about exposure therapy in a massage clinic setting. But, if we buy into misconceptions we’re less likely to use something that’s REALLY effective, however, we should be using this with all the confidence that its evidence base deserves.
http://themtdc.com/wp-content/uploads/Articles-of-57.png400600Jamie Johnstonhttp://themtdc.com/wp-content/uploads/logo.svgJamie Johnston2020-06-06 22:21:222026-04-22 20:31:20Articles Of The Week June 7, 2020
As different parts of the world start to come out of isolation and begin pondering what work will look like, we have to acknowledge that things are going to be different…forever.
I’ve seen the question asked “who in this profession is going to make it”?
There was some debate around this and a few comments I’ve seen are things like:
“massage is a luxury, only those who have money are coming back”
“Only medical massage therapists will pull through”
“Only those who work in a clinical setting will be able to recover”
Well, the reality is, none of that is true and it quite frankly doesn’t matter what setting you work in.
This is what determines who will be successful after this pandemic, or any other one we may face down the road.
Using Trust To Create Sustainability
It’s not often I say this, but I have to give some kudos to our college.
While they put in the effort to put together a return to work document1 for our reference and give us some direction on how we should handle things, there was a central point they made in the direction.
Build trust with your patients.
They outlined cleaning procedures, PPE protocols, and new consent instructions, yet at the heart of it all was the direction to do or wear these things in front of your patient, if for no other reason than to build their trust in you as the healthcare professional.
It’s honestly the first time I’ve seen something like this from our regulatory body, and I applaud them for it.
Along with this was a perspective piece written in the New England Journal of Medicine2, although it was written from a doctor’s perspective, I couldn’t help but see how this is applicable to us as therapists.
In the article, they talk about the importance of relying on evidence-based practice. While this is always important, at a time like this that importance is amplified as patients and therapists alike could be making decisions based on fear and emotion, which in turn can result in falling prey to cognitive bias and making therapeutic errors.
Since our role as therapists is to provide safe, effective care we need to have what this article calls a “healthy skepticism” and keep our clinical equipoise when considering any intervention.
If we don’t retain this healthy skepticism we run the risk of relying on personal anecdotes where all too often in our profession we see people saying things like “I know it works because I’ve seen it work” while at the same time refuting and even sometimes refusing to accept research into their practice.
When things like this happen it is usually a result of what the article calls “the intense desire to try new and unproven remedies”. Think about how this applies to many of the continuing education courses we see in our profession. Many of them don’t have research to prove their unsubstantiated claims and yet we look to try this new intervention possibly making therapeutic errors.
Of course, all done with the absolute best of intention trying to help our patients.
If we are going to be successful once this is all over and we want to build sustainability in our practice, this has to change.
As tough as this whole shutdown has been, it has also created an opportunity for change. As we move forward trying to build trust with our patients while also gaining sustainability in this profession, there’s one other golden nugget we need to look at.
Therapeutic Alliance
There are many things that influence our treatment outcomes that go well beyond whatever our favourite modality is.
Some of these are referred to as non-specific or contextual factors.3
Part of these factors is the therapeutic alliance we have with our patients which can be defined as:
“The working rapport or positive social connection between patient and therapist”3
And
“Established between therapist and client through collaboration, communication, therapist empathy, and mutual respect”4
This systematic review4 showed there were 8 major themes associated with therapeutic alliance:
Congruence
Connectedness
Communication
Expectation
Influencing factors
Individualized therapy
Partnership
Roles and responsibilities
Now, we could probably write an entire article on each one of these 8 themes, how it applies to us in practice, and how we could effectively use them, but let’s leave that for a later date.
For now, let’s just consider what was most important to the patients.
Of those 8 themes the most important determinants of a therapeutic alliance in the eyes of the patient were:
Communication
Interpersonal aspects
Partnership
Roles and responsibilities
Another thing the review showed was both patient and therapist agree that effective communication improved treatment adherence. They also found that agreement on goals and tasks, sense of connectedness, positive feedback, genuine interest, individualized care, trust in the therapist, and feeling empowered were all important predictors of exercise or homecare adherence.
The way we communicate, listening, sending appropriate messages and words of encouragement actually has an influence on reduction in pain.4 However, it’s important to note that making inappropriate comments can actually make patient’s symptoms worse (which also demonstrates why communication is so important in the patient’s eyes).
They also came to understand a few more sub-categories important to build this alliance. Included are humour (I can only use a limited supply of this as my sense of humour is pretty offside), emotional intelligence, appreciation, honesty, clarity of information and feedback, support and follow up.
Are you as excited as I am when looking at these lists?
I’m sure most of us are already doing many of these things in our practice, but how often do we practice them, get better at them, take a course on them? While they are deemed “soft skills” the research is showing us these things should be at the forefront of our practice.
And the great thing…we get to spend more time with our patients than most other manual therapists and we can literally practice most of these things during our treatments. This was another one of the things that positively influenced outcomes, the amount of time spent with the patient along with warm, empathic interaction!4 So while there was no way for us to predict this pandemic, there are ways for us to create sustainability in our career. Massage therapy as a profession isn’t going anywhere, people will still need help, and still want to be touched in a therapeutic way. Unfortunately, some clinics won’t recover from this which is an absolute travesty that no one deserved to go through. But the best way to create sustainability is by enhancing and developing strong therapeutic relationships with our patients. With that strong relationship, should something like this ever happen again, those patients will be waiting for your clinic doors to open again because they trust you will do what’s best for them. As we start our clinics up again, while it won’t be the same, there is a genuine opportunity to start building that trust again while creating sustainability in your practice.
Zagury-Orly I, Schwartzstein RM. Covid-19—A Reminder to Reason. New England Journal of Medicine. 2020 Apr 28
Fuentes J, Armijo-Olivo S, Funabashi M, Miciak M, Dick B, Warren S, Rashiq S, Magee DJ, Gross DP. Enhanced therapeutic alliance modulates pain intensity and muscle pain sensitivity in patients with chronic low back pain: an experimental controlled study. Physical therapy. 2014 Apr 1;94(4):477-89.
Babatunde F, MacDermid J, MacIntyre N. Characteristics of therapeutic alliance in musculoskeletal physiotherapy and occupational therapy practice: a scoping review of the literature. BMC health services research. 2017 Dec;17(1):375.
http://themtdc.com/wp-content/uploads/Untitled-design-64-2.png6381036Jamie Johnstonhttp://themtdc.com/wp-content/uploads/logo.svgJamie Johnston2020-06-02 07:53:212026-04-22 20:30:04Creating Sustainability With Therapeutic Alliance
We did an article on this topic a couple weeks ago, so it’s great to see the awareness being raised around this topic. There is little correlation to “weak glutes” being the reason for a person’s low back pain, so let’s build resilience with people rather than preaching false narratives.
For those of you who treat kids on a regular basis, I’m sure you’ve seen the importance of having the parents appropriately on board with treatments. However, sometimes they may be sending the wrong message, which can make for a difficult conversation. So, here are some tips on how to manage those conversations.
This could be one of the most beneficial videos you could share with your patients regarding back pain (especially if they’re considering surgery). I’m hoping this will change a lot of minds having people choose rehab over surgery.
Love this pain analogy and it’s another one you should DEFINITELY share with your patients. Sometimes we experience pain when our “cup” gets too full, or we can’t get a bigger “cup”. The things happening around this can influence the amount of pain we feel and in turn change how we are managing things in life. So maybe we either need a bigger cup, or decrease what’s in the cup.
This is a really important topic for both patient and therapist. Everyone involved in this podcast is doing great work to benefit both patients and therapists, so this is WELL worth the listen.
http://themtdc.com/wp-content/uploads/Articles-of-55.png400600Jamie Johnstonhttp://themtdc.com/wp-content/uploads/logo.svgJamie Johnston2020-05-30 16:14:322026-04-22 20:30:04Articles Of The Week May 31, 2020
The Prone Press Up is one of the best ways to prevent and treat acute low back pain. Even if you get a massage, adjustment/manipulation, or other treatment in a clinic, you still need to maintain the improvement at home (unless you want to pay for a passive solution forever).
A patient is more likely to get better if they do a high dosage of repetitions throughout the day of whatever resets their system. If it hurts, they’re less likely to dose or to get to end range. Here are some of my favorite ways to make the prone press up pain-free or to eliminate the perception of tightness at end range
Any or all of these strategies should make the press up pain-free or as comfortable as possible so a high dosage should be easier to accomplish.
http://themtdc.com/wp-content/uploads/Press-Up-Massage-Therapy.png6871036Erson Religiosohttp://themtdc.com/wp-content/uploads/logo.svgErson Religioso2020-05-26 07:48:422026-04-22 20:30:04Level Up The Prone Press Up
I hope this lockdown has brought about some positive change for most of us. Maybe we’ve learned a new skill, made a new connection, developed a hobby, or just come to appreciate our work more. Perhaps there are also lessons to be learned as therapists who are helping people with pain as a result as well.
We’ve all experienced some change during this pandemic both professionally and personally. I know some of our colleagues have been doing some work online with patients and it’s interesting to see how one mental health therapist noticed a difference in doing online appointments.
Quite often when helping a patient and providing homecare, it may be necessary for them to change a certain behavior. This can be pretty tough, but there is science behind why it’s tough. Here are five reasons why.
As we start returning to work, we may be seeing some people who have taken up running or some other exercise during the pandemic. As a result we may see some people coming in with some tendinopathy issues. Here’s some advice on how we can help with lower limb tendinopathies.
This generous offer has three different resources to help you grow your business during this pandemic. It might be good to use as things are starting up in some areas.
http://themtdc.com/wp-content/uploads/Articles-of-53-1.png400600Jamie Johnstonhttp://themtdc.com/wp-content/uploads/logo.svgJamie Johnston2020-05-23 17:19:292026-04-22 20:30:04Articles Of The Week May 24, 2020
Whether rehab exercises should be painful or not has become a recent topic of much discussion. As we have started to value the role of (optimal) loading in rehab, and that we can get patients back to moving and loading pretty early in the rehab process, we have also got to appreciate that this is unlikely to happen without experiencing any pain.
If you have any type of understanding about pain then the simple question of “should we use painful exercise?” suddenly might not look so simple!
Rather than a simple yes or no, there are a bunch of questions to be answered, such as how much pain is OK? Who may or may not benefit? And what is the best way to manage the process? Especially if all does not go to plan!
Research
From a data standpoint it would be great if we had have something that we can use to guide us here. Low and behold we do, and its open access.
This systematic review and meta analysis looked at 9 trials in which varying degrees of painful exercise were used. They found that painful exercise did NOT result in statistically worse outcomes across a short, medium or long term follow up. There was a small statistical benefit in the short-term for painful exercises as highlighted by the standardised mean difference of around 0.2 (SMD = effect size for a meta analysis). So from a research standpoint this is positive news.
One thing to note here from a clinical standpoint is, that using painful exercise is no GUARANTEE that it will have a positive effect for your patient. All statistical tests only give us the PROBABILITY of an effect, so the likelihood is that it will, but when we look at the confidence intervals (measure of variability) for the mean SMD for painful exercise, for the majority of the studies we can also see that they cross into a negative effect and in some of the studies quite substantially.
The variable effect of exercise on pain (although over a shorter time frame) was also shown by O Neill et al’s recent look at the acute effects of isometrics *Here*. Although, of course, isometric exercise and painful exercise is not the same thing, the point here is the highlighting of the variable effects from exercise. For patients with higher baseline pain isometrics actually increased their pain post exercise and this is the benefit of looking at individual responders within a study not just the group average. Those with lower pain at baseline seemed to receive more analgesia from isometric exercise.
BUT at the very least I think we can say that the likelihood is that it will not have detrimental effect. So as rehab can often be painful we can be reasonably confident but without seeing painful exercise as some sort of fire and forget panacea and also appreciate the individual nature of pain.
We could debate the mechanisms of HOW painful exercise might work from pain habituation to conditioned pain modulation and perceptual mechanisms but in essence we don’t really know at this point in time and this might be different or in different combinations for different people.
Benefits
The benefits can be both physical AND psychological.
Firstly, it allows patients to get in MORE exercise. If they are not being limited by pain (or pain contingent if we are being fancy :) then they can get a greater dosing than if they stopped due to it being painful. It is important to add though that we currently don’t know what optimal dosing is for exercise having an effect on pain!
Secondly, it sends the message that hurt does not equal harm. The problem can be painful and still settle down if managed in the right way. This may give people a new insight into their pain and how they can manage it.
Pain self-efficacy may also be built experientially, so using painful exercise as a tool might be an option to help do this.
Clinical Application
So it’s great to have some objective data on this subject, but as we know getting that into clinical application is not always straightforward.
Firstly don’t be afraid of some pain! The likelihood is that it won’t cause a worse outcome. But as we are dealing with thinking, feeling HUMANS, it is OF COURSE not as simple as this, but more on that later.
One of the issues with always looking to be pain free with exercise or continually treating pain, is what does that say ABOUT pain? On one hand we are telling people hurt does not mean harm but our actions might not be saying the same thing. If pain is OK, if it is normal then in the process of getting it better we might have to endure a little bit of it.
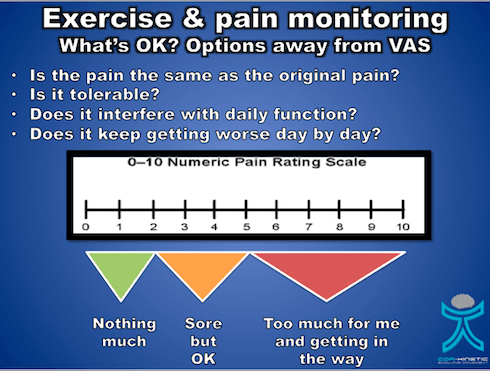
But how much is OK is a key question? Studies that have allowed painful exercise have ranged from not increasing baseline symptoms during or post exercise up to 5/10 on the VAS.
We know the limitations of the VAS as a REALLY subjective scale so perhaps we could introduce the idea of pain being tolerable or intolerable rather than a numerical score.
Now tolerable might be a bit sore but it does not really get in the way. Intolerable might be thought of as getting in the way of our daily activates, maybe having an effect on our sleep and generally making life a bit miserable. This is going to be different for different folk so hence why the concept of tolerable becomes important.
We would also like to know how the pain is settling down. So pain that is not really calming down after the exercise stimulus or keeps on getting progressively worse over a number of days as the exercises are performed is probably not a great idea. We would like to see a nice stimulus response with only slight increases above baseline (tolerable remember : ) that calms down gradually over 24-36 hours, quite similar to delayed onset muscle soreness (DOMS)
So on the issue of DOMS, it is important to identify if the increase in pain is actually the same as the original symptom. Post exercise soreness is quite normal but for those that are unaccustomed to exercise this might not be recognisable especially for a currently painful area. Defining what is pain and what is soreness might be a good sense making exercise for some patients. Although we don’t know that progressive overload is required with exercise in rehab, it probably ia a good idea, so having some sort of tolerable baseline for patients to progress or regress from is a great idea too. This is also might have an effect their self efficacy using exercise too which, of course, is a bonus.
Pain Is Not The Only Issue
Potentially the most problematic area with painful exercise, and one that is really under discussed, may be more about the psychological aspects that are associated with the pain and how they can affect the person. One of the best prognostic factors for recovery in a number of body areas appears to be pain self efficacy, *here* is a recent paper from Chester et al and also from Foster et al *here* Pain self efficacy, something I have written about before also *here*, is the ability to carry on normal functioning despite of pain. It is important to note that those with higher pain self efficacy also tend to adhere to exercise better.
So someone’s pain self efficacy is going to be a KEY factor in whether they are able to tolerate having pain and being able to carry on functioning which maybe a fundamental skill at the heart of painful exercise especially if it can take 24-36 hrs to settle.
Predicted outcome is another key prognostic factor and if someone believes that increased pain will result in a negative outcome then this could have a negative effect on the actual outcome.
Jack et al *here* found that the number one reason for poor adherence to exercise programs was that people did not want to make the problem worse. So painful exercise coupled with negative beliefs about pain, low pain self efficacy and a poor predicted outcome may not sit well together.
Firstly you could screen people for these factors if you feel they are required. We have tools such the Pain Self Efficacy Questionnaire (PSEQ) and the shorter version the PSEQ-2.
One caveat with using questionnaires, in my opinion : ), is it does allow us to get a score to assess confidence and resilience in managing pain but it perhaps does not tell us about things that are specific to our patients. So being able to weave this into a good subjective that teases these more personal parts of the narrative out is a must.
Also ASK about their expected outcome from the treatment and what would it mean to you if it was painful.
“Do you feel like this exercise will work for you?”
“Do you have any concerns about doing this exercise?”
It might be that someone tells you that they have tried exercises before and they did not work or that they feel it might make the issue worse, especially if it hurts.
It might also be important to discuss with ALL patients what their beliefs are around pain. These might be that pain indicates they are doing more damage to their bodies or they will not be able to work because they have pain or implications for future functioning. It can often be what the pain MEANS to the patient that is the real issue rather than just the sensation of the pain itself.
A key factor to remember is regardless of whether painful exercise is positive or no worse than non painful exercise, a negative belief may stop your patient from exercising
Education
One of the most powerful tools we have at our disposal is EDUCATION, I am not always a huge fan of this term as it can imply a teacher pupil relationship. But in order to provide effective education to people we first have to build rapport and then understand what they may need to know more about.
We can educate on a range of things from the effectiveness of exercise for many issues, that painful exercise is often not detrimental, that pain self efficacy is an important prognostic factor and what pain may actually mean and its relationship with physical damage. It may also be worth talking about the process and what to expect, and often that it is a process of trial and error to get the right level and desired response.
This has to start with understanding the patient, their history and belief structure.
Where You Start Is Not Where You Have To Finish
Do we have to jump straight into painful exercise? I don’t think so. It is not REQUIRED but it is also not harmful.
An important point to make is that for someone with very negative beliefs about pain, reduced pain self efficacy and poor beliefs about the outcome, challenging them right off the bat with painful exercise might not always be the best thing to do. As they build trust in you and confidence in their bodies then pushing into pain progressively might sometimes be a better route.
We know that giving people the option to avoid pain can actually maintain pain avoidance, so whilst not advocating avoidance behaviour confronting these things may take a little time, confidence and education, especially if the person has a lot of negative pain and avoidance based beliefs.
Those that persist in doing painful things that have NOT provide a therapeutic effect may benefit from non painful exercise for a while too. If you feel that pushing into pain has not given the desired response when looking at their history then a break or change in dosage could be just the ticket.
Those with higher levels of pain at baseline on average seem to have worse clinical outcomes so this might also lead me to reason that maintaining this level of pain through exercise might not always be a good idea.
There are no real hard and fast rules here only individuals and individual considerations.
What If It All Goes Wrong???
This is where self efficacy may come into its own. Empowering your patients to self manage maybe valuable in the exercise process.
As we hopefully have told the patient BEFORE they embark on an exercise program I can often be trial and error. Have we enabled our patients to adapt their exercise dosage if it goes a bit wrong? *Here*is a short piece on dosage in rehab
So do your patients know what to look out for in terms of symptoms?
Do they know how to adjust the dosage? This could be in exercise frequency, intensity and time, sets and reps (volume).
Are they able to contact you to ask questions? Do they know this?
I think these are all required aspects of pushing into pain.
A patient I saw last week had religiously persisted at pushing into his painful rehab exercises every 48hrs. He believed if he did what he was told he would get better (the trust!). But after 3 months there was not the desired outcome. In this case he was given no indication what to do if this happened, just blind faith on all sides that he would get better.
Key Points
Painful exercise DOES NOT produce worse outcomes from the research we have
Research does not guarantee your patients response to painful exercise
It is not just about the PAIN sensation! What does the pain mean and how does it affect behaviour such as exercise adherence?
Pain self efficacy and predicted outcome are important psychological measures and can be discussed and measured
Think about education around the exercise and the pain response
It does not need to start with painful exercise!
Empower your patients to self manage
http://themtdc.com/wp-content/uploads/Massage-Therapy-Painful-Rehab.png6871036Ben Cormackhttp://themtdc.com/wp-content/uploads/logo.svgBen Cormack2020-05-18 20:07:562026-04-22 20:30:05Painful Exercise In Rehab – Yes, No, Or A Lot To Think About
We may request cookies to be set on your device. We use cookies to let us know when you visit our websites, how you interact with us, to enrich your user experience, and to customize your relationship with our website.
Click on the different category headings to find out more. You can also change some of your preferences. Note that blocking some types of cookies may impact your experience on our websites and the services we are able to offer.
Essential Website Cookies
These cookies are strictly necessary to provide you with services available through our website and to use some of its features.
Because these cookies are strictly necessary to deliver the website, refusing them will have impact how our site functions. You always can block or delete cookies by changing your browser settings and force blocking all cookies on this website. But this will always prompt you to accept/refuse cookies when revisiting our site.
We fully respect if you want to refuse cookies but to avoid asking you again and again kindly allow us to store a cookie for that. You are free to opt out any time or opt in for other cookies to get a better experience. If you refuse cookies we will remove all set cookies in our domain.
We provide you with a list of stored cookies on your computer in our domain so you can check what we stored. Due to security reasons we are not able to show or modify cookies from other domains. You can check these in your browser security settings.
Other external services
We also use different external services like Google Webfonts, Google Maps, and external Video providers. Since these providers may collect personal data like your IP address we allow you to block them here. Please be aware that this might heavily reduce the functionality and appearance of our site. Changes will take effect once you reload the page.
Google Webfont Settings:
Google Map Settings:
Google reCaptcha Settings:
Vimeo and Youtube video embeds:
Privacy Policy
You can read about our cookies and privacy settings in detail on our Privacy Policy Page.