Resilience is a term used more and more by therapists, some might suggest it is a buzz word, so I wanted to put down my thoughts about this complex subject. I have wanted to write this blog for a while and the struggle I have had here is to keep it bloggy, not too academic and above all not too long! I have tried to strike a balance between research and also some personal experiences of resilience I have collected.
Before we get into it, there are 3 main points I would like to make in this blog.
Firstly, resilience is NOT about manning (or womaning) up, it is NOT SIMPLY about just keeping going. It’s a flexible, adaptable state that recognizes the importance of specific actions, mental or physical, that have a positive impact on life.
Secondly, resilience is not a binary state between resilience and not resilient. It is a continuum that we move along dependent on a balance of internal and external factors.
Thirdly that resilience looks and feels different between people. What you may regard as resilience MAY NOT be the same as the person you are working with.
What Is Resilience?
Resilience is defined by Sturgeon *HERE* as,
“Maintenance of positive physical and emotional functioning in spite of significant difficulty or challenge”
So resilience is both a physical and a psychological thing. It is important that we don’t separate the two, however (much like pain!). Although physical things often signify resilience, they require a strong psychological component to achieve and also give a lot of psychological benefits.
This is also a good read *HERE*
Karoly *HERE* defines resilience as (2006) as
“Effective functioning despite the exposure to stressful circumstances and internal distress”
Both definitions use the word FUNCTIONING and ‘in spite’ or ‘despite’ of pain.
This makes resilience a REALLY individual thing that looks quite different between different folk. We should not make the mistake of assuming what signifies resilience to us is the same as someone else’s.
Pain is definitely a stressful circumstance for many, and it really becomes a problem when it interrupts our functioning. Focusing on the stressor, pain, however, could be part of this problem. Essentially resilience should be seen as a problem of function rather than pain. This is an important distinction, as identification and engagement of functions must form the key focus (IMO) rather than the focus that many can have (patient & therapist), pain itself.
Sturgeon writes;
”Attempts to control a chronic stressor like chronic pain are often counterproductive and can magnify the negative effects of the stressor”
Sustainability
Goubert & Trompetter *HERE* introduce the concept of sustainability; this is defined as:
“ability of a person to move towards long-term positive outcomes in life in the presence of adversity”
Here is a nice graphic outlining sustainability vs recovery from their paper.

Sustainability targets the PERSON in pain rather than the pain itself. Perhaps sometimes the focus can be on the pain going away before function is resumed, but we could view this the other way around with functioning through resilience being the first step.
The concept of sustainability is important, as it looks more at positive traits rather than risk factors. This is a bit like Antonovsky’s Salutogenic approach *HERE* that focuses on health rather than disease.
So to sum up resilience, it is about PEOPLE and FUNCTION more than pain and withstanding pain (IMO). Working through ANY pain or injury will require some element of resilience. Acute back pain, one of the most prevalent painful issues, probably exemplifies the need for resilience, with the first-line treatment for back pain being the advice to remain active and engage in your normal activities *HERE*.
Perhaps initial resilience may mediate the transition to more persistent pain states?
Adaptability & Flexibility
Resilience should not be seen as a brick wall. A resilient person is not simply a cold piece of rock impervious to any stressor. It is not about toughness, it is instead a flexible and adaptive state.
It could be quite the opposite, in that resilient people might be willing to seek out help instead of the strong silent type who may not be as resilient as they appear externally, unable to appear weak or vulnerable by asking for help. Resilience may be the ability to open the pressure valve and allow the excess to release and lower the stress by identifying things that allow them to do this or provide a balance with stressful situations.
Pain Relief Vs Resilience
Therapy has long been driven by pain relief, and whilst there is no doubt this is a reason why people seek care, they also seek care because pain is disrupting their lives and functioning, perhaps even more so for this reason.
This paper by Ferrara found that disability was a greater reason for care-seeking than pain intensity *HERE*
So perhaps to understand resilience we have to understand to understand our patients functioning and what THEY view as key markers to signify resilience. Traditionally VAS scales and physical measures such as strength have been used to measure clinical success. But do these measures capture valued activities and what resilience might mean for the person? Perhaps not. This paper looks at this subject of what is measured clinically vs peoples ACTUAL goals *HERE*.
So in order to help people BE resilient a good place to start is to find out more about how THEY view resilience, what defines their effective functioning and how we might bridge the gap between their current and desired states.
Resilience Is Personal
Valued activities may provide balance during stressful situations. Especially people that suffer from persistent pain can lose sight of things they used to do and the things that might define resilience. These are the people that may need a guide or a coach to find some meaning or goal again.
The sustained engagement in cherished activities, or stuff that MEANS stuff, seems to be a huge marker of resilience. To get a better idea of some of the meaningful activities, I asked some of the folk on social media (not in-depth research I know) to let me know some of the things they found important during painful times.
Exercise seems to be a really important sign of resilience for people and it was amazing to hear so many success stories against some pretty adverse situations. On a side note, communicating patient success stories to other patients, delivered at the right time and in the right way, can be a very powerful tool in my experience.
- Weightlifting
- Capoeira
- Yoga
- Pilates
- Boxing
- Bike riding
- Crossfit
- Running
- Walking
- Bouldering
- Various sports
- Gymnastics
- Dancing
- Making things
- Hiking
Work also featured heavily. Just day to day functioning seemed important. Much like exercise, our working lives are pretty varied from being a therapist to nursing to simply driving. The concept of family also featured heavily with helping and providing for them forming an important part of resilience for many.
Resilience seems to be a rich tapestry of different things. The clinical implication of this is being able to effectively listen and ask a few questions that allow us to find out more about what activities may signify resilience and then be able to guide someone towards them and also provide planning and support for engagement.
Here are some example questions I use:
“What would your perfect day without pain look like?”
“What have you stopped doing because of the pain?”
“Are there things you feel are important that you avoid because of the pain?”
I also picked out some quotes. I have not used any names : )
“For many years, my default position was to isolate myself, try to power through, and go out of my way not to seek out resources or strategies. I thought that was the way I was supposed to do it; “man up” and push through. For me, I think I discovered (still am) resilience when I learned about acceptance. Getting to acceptance, and I think I still struggle with that a bit to this day, was a difficult time as I had to admit that I could not do this on my own. I hated that feeling”
“Resilience is in all of us, but sometimes we need a guide to help us find our path forward, but there is always a path forward”
“I would say the thing that made me the most resilient was asking for help. From my mentors, friends, counselors and family. Vulnerability helped me be more resilient”
“I love riding my bike but on a steep hill climb, my pain would escalate 10 fold. I persisted and after 30 mins or so of cycling it would go back down to normal levels. The bike ride was more important for my mental well being than the back pain maybe that is why I persisted”
“Resilience for me is knowing that there are things you can and can’t control and you put energy and focus into those things you can control/accept”
“Resilience is I get up every day and work with injuries on others. Sometimes leaving bed is the hardest part”
It could be balancing the stressful parts of life with things that bring us happiness and joy is most important and when we lose this balance is when we start to become more vulnerable and our job may be to help with this process.
What Components Make Up Resilience?
Both Sturgeon and Goubert outline some positive elements AND some risk factors involved in resilience.
Lets first start with the positive elements.
Optimism & Positive Emotions
Optimism appears to be a key characteristic, with optimism being related to lower levels of pain and this may support why predicted expectations are related to outcomes. Optimism should be viewed both from a clinician and patient viewpoint and withou,t doubt both viewpoint will interact within the ‘third space’.
Here are some good papers *HERE* & *HERE*
Questions we can ask ourselves:
- Are you a generally optimistic clinician/person?
- How optimistic are you about a positive outcome?
- Do you discuss what a positive outcome might look like, especially in regards to improved function?
- Can we highlight positive aspects from the person’s story/history, previous positive experiences to be optimistic about?
Although it is important to not seem disingenuous, the need for positivity and a positive emotional perspective on life and activity should be highlighted, although this should probably come after a validation of normal negative responses to a tough situation such as persisting pain.
I feel it is also important to highlight the negative aspects of negative thinking and behaviour.
Pain Acceptance & Sustained Engagement In Valued Activities
Pain acceptance is defined as acknowledging that one has pain, stopping attempts to control pain, and learning to live a richer life in spite of pain. This in turn can lead to more engagement in valued activities.
Sturgeon writes
“individuals with greater levels of activity engagement are better able to bolster their positive emotions through sustained pursuit of valued activities despite their pain”
This appears to be a key factor, both highlighted in the research and also in the in depth qualitative research I performed above on social media ; )
Social Support
People who actively seek out social support seem to have lower levels of pain. We know from work such as Riikka Holopainen’s *HERE* that people with persisting pain reported that their circle of life had shrunk and they had given up doing things they used to enjoy.
Pain can interrupt positive social interactions that are important for resilience, however, pain can also narrow our ability to identify these positive social interactions and positive resilience resources in general.
Risk Factors
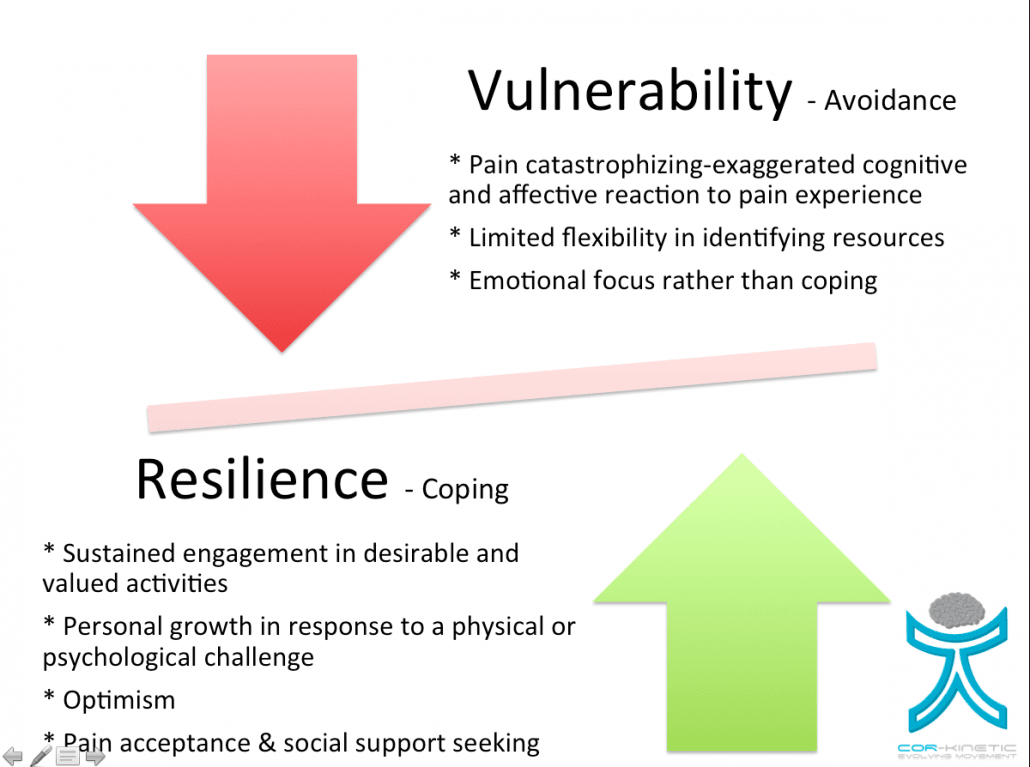
Pain Catastrophisation & Avoidance
Higher levels of pain catastrophizing and fear are linked to higher levels of pain and pain catastrophizing can also lead to ineffective coping strategies such as an avoidance approach to coping. This behaviour is consistent with the affective-motivational side of pain that can often motivate people to avoid things such as social interactions and physical activities. Essentially this can limit the enjoyment and positive aspects gained from valued activities, often for fear of pain, and can reduce resilience behaviours. This prolonged avoidance can also lead to depression and disability.
I feel it is important to highlight avoidant approaches and also help someone to rationalise if they are actually helpful for them or not.
But it is also important NOT to simply label people avoiders. Avoidance like all things is complex. Some activities may display avoidance behaviours whilst other things are engaged in. It is a touch harsh to take an area of someone’s life they are struggling with and use it to define them.
Resilience Or Vulnerability
We must be mindful that resilience does not appear to be a stable state. People are not simply resilient or vulnera,ble. Instead they appear to have components of both aspects co-existing in a sort of balancing act. Sometimes we maybe more susceptible to vulnerability, even the most resilient is resilient until they are not. We may also be vulnerable in some areas of our lives but not in others. We could be physically resilient but emotionally vulnerable or the other way around. It could switch from day to day. The one thing we know about the experience of pain, and all the dimensions that go into it, is that it pain is predictably unpredictable.
Resilience should really be seen as a continuum. Different injuries may require different levels of resilience and the person will have a current resiliency state dependent on many factors in their life. Some people may be super resilient or the injury type or state may not require much resilience. As with all painful problems, this relies on clinical reasoning to apply the right care at the right time.
Take Homes
- Resilience IS NOT TOUGHNESS
- Resilience is about adaptability and physical and psychological flexibility
- Resilience lies on a continuum
- Resilience looks and feels different to different people
- Optimism is key
- Sustained engagement in valued activities is key
- Pain catastrophization and avoidance behaviour are risk factors
