Beliefs, Communication, And How This Impacts Our Patients
I’m sure I’m not alone when I say I’ve seen some horrific things in my practice.
Now, when I say this, it’s not in the sense of major catastrophic injuries, or gory blood scenes, or something like that.
What I’m referring to is what I’ve seen and heard from patients as a result of what another well-meaning practitioner said to them.
A patient comes in, sits down, and starts crying because another therapist told them they will never get better.
Another person who has been dealing with chronic pain for several years comes in and equates the pain they’re feeling in their back to a “rib being out”, or “their S.I. Joint is out again”.
And in the more extreme ranges someone giving up a career they love, in exchange for a job they hate because two people told them they would never be able to do their job again because of the surgery they just went through. In fact, told them if they continued doing the job they loved (and were very successful at), the surgery they just had would pale in comparison to the one they would need.
While I know none of these practitioners would intentionally have someone change their job, believe they won’t get better, or would constantly relate pain many years later to a simple biomechanical diagnosis, the reality is, their words changed people’s lives.
And not for the better!
So, why then does this happen? Why are these enduring effects of words having such a dramatic impact on patients? And, more importantly, how do we stop this?
When Well-Meaning Beliefs Go Wrong
When we say “well-meaning” practitioners I do believe it’s just that. I doubt there are many out there legitimately trying to say harmful things to their patients (although I do believe there are some who use less than scrupulous language as part of the rebooking process).
So, when we have these well-meaning professionals saying things to patients, part of why they are saying the things they are is because they truly believe it (even if modern research refutes it). Part of the issue is when these belief systems are passed on to our patients it can have a lasting effect in a negative way.
Unfortunately, many of these belief systems can come from continuing education courses that haven’t been updated in years and are still preaching these outdated belief systems.
A great systematic review (1) looked at several medical and paramedical professions to look at how their belief systems, (including biomedical and biopsychosocial treatment, fear-avoidance beliefs, and attitudes) affected patient behaviours.
There were several things that stood out to me reading through this(1):
- High levels of fear-avoidance in practitioners are related to the same fear-avoidance in patients.
- Practitioner beliefs are associated with the education they give patients.
- Practitioners with a more biomechanical base are more likely to advise acute pain patients to limit work and physical activity.
- Those with high fear-avoidance beliefs are more likely to recommend bed rest (which we know is not good for low back pain) and are also more likely to recommend this if seen in a media campaign.
Now I realize it probably sounds like we’re bashing anything related to biomechanical explanations here but honestly we’re not.
As we have said so many times over the years, biomechanics are still important, it’s just one piece of the puzzle. What I’m taking from this review is that if we’re strictly relying on biomechanical explanations we’re more likely to also cling to fear-avoidance beliefs as well, which isn’t doing our patients any good.
Part of the problem here is that if a practitioner has these beliefs, they get passed on to the patients we see. One of the major issues with this (as pointed out in the review)(1) is these beliefs result in persistent disability but not necessarily a change in pain.
So, if these beliefs are held, the patient’s pain won’t always change, but there is an increase in disability. Imagine your patients coming in for care and strictly because of a belief system, not only does their pain not get any better, but they become more limited in the things they can do.
In light of all this information, I look back and think about early in my career and how I was saying very similar things to my patients. There comes a time when we have to sit back and ask ourselves whether the information we are conveying is correct, but also, is it in their best interest?
This review showed that even though some health care professionals believed in the biopsychosocial framework (it was originally introduced over 40 years ago), they were still operating from a biomedical orientation. In the case of doctors, they understood how important psychosocial factors can be yet, they lack the time to properly integrate this into practice.
So, while I look back on my career and cringe at some of the things I used to say, I look at this information and see how beneficial this is for us as Massage Therapists. If we embrace new research and change our beliefs, we not only have the time to spend with our patients, we have the opportunity to create lasting change for what they are going through.
Words Matter!
So, now that we understand the influence of both the patient and therapist beliefs, the question remains, where did these beliefs come from?
Quite often these beliefs are because of lived experience, observing others in pain, or things that have been told to them throughout their life. A big influence was just not having a framework or a reference of what they should do when experiencing pain.(2)
All too often we see patients going to Dr. Google for advice, however, while this is usually looked at cautiously, people do place higher importance on the advice of friends and family.(2) While people would often seek out care from a health care professional, they would sometimes reject the advice given as they questioned their competence, and would even keep their own beliefs if it conflicted with the advice of a professional.
Now, this isn’t necessarily a bad thing because there’s nothing wrong with a patient using their own intuition to choose what course of action is best for them. It’s important for patients to feel confident in the information being presented to them, in fact, it’s even possible for their symptoms to be influenced by their interpretation of the education they are given.(2)
However, even if we believe we are giving them a very simple explanation of what is happening, there can be an enduring impact. I can now hear my mother’s voice resonating from my childhood and what she would say every time my brother and I would fight: “it’s not what you say, it’s how you say it!”
This paper has several examples of the lasting effect of what we say, which I think are important to highlight.
When a doctor gave a simple diagnosis of a sprain in an attempt to decrease the seriousness of the injury, the patient understood this to mean they had moved in such a way they had strained the muscle and they would make it worse by continuing to move the same way.
In the case of a person getting help from an orthopedic specialist, the result was well…horrific:
[The orthopedic specialist] looked at my back MRIs for a little while and turned around with a grin on his face and said, “You’re a builder, aren’t you?” and I said, “Yes,” and he said, “You’re [expletive], ha ha ha,” and went back to his computer again…. So, you know, I think that was his rather odd specialist way of breaking the news to me that I wouldn’t be working as a builder for very long…. Every time I felt a little bit wrong [after that], I started to sort of add it up in my head. And then my usual way of thinking, “Oh, that’s fine, that’s nothing, that’ll go away, that’s not major enough to stop me working, I’ll carry on [changed]”…him saying that was definitely the point, because I probably would have just carried on(2)
This person actually ended up changing careers as a result of what was said to them! Sadly as I mentioned, I’ve seen the same result in practice as well.
Another example that stood out to me in the same paper was equally as life-altering:
Basically all I’ve kind of been told to do by physios is to work on my core…I’ve been tested by various different physios, and Pilates, and I’m apparently ridiculously weak…. I had an abortion because I didn’t think I could have a baby. I didn’t think I could handle it…carrying it, and having extra weight on my stomach(2)
Can you imagine what this woman went through dealing with this?
Again, I’m sure these were well-meaning practitioners but when our communication is focused more on the things we can’t do as opposed to the things we should do can have compounding long-term effects. If we shift this line of thinking and encourage movement, provide reassurance, and show people how they are safe to remain active it can (and most likely will) have the reverse effect of the quoted stories we shared.
While many practitioners have a belief in the biopsychosocial model, many are still using biomechanical explanations of tissue damage, etc in an attempt to help their patients. As we have seen this can be detrimental to the patients well being. So it’s important to have a discussion around how to change these beliefs in practitioners. Many of us went through college and learned these things (I know I learned many of these explanations in school) and unfortunately, there are many continuing education courses still offering these kinds of explanations. This becomes our responsibility as a profession to change this, and really it starts with each one of us. It doesn’t even mean you have to spend thousands on new courses, it can mean just reading blogs like this, or a new research paper a week (it doesn’t take that long I promise), because we must change our beliefs in order to have a better impact on the people we are seeing in practice. When our beliefs (and our messaging) start to change we can slowly change our patient’s beliefs for better outcomes. Then, hopefully…hopefully, patients feel safe to return to their careers or have babies, or just return to an activity they love.
References
- Darlow B, Fullen BM, Dean S, Hurley DA, Baxter GD, Dowell A. The association between health care professional attitudes and beliefs and the attitudes and beliefs, clinical management, and outcomes of patients with low back pain: a systematic review. European Journal of Pain. 2012 Jan;16(1):3-1
- Darlow B, Dowell A, Baxter GD, Mathieson F, Perry M, Dean S. The enduring impact of what clinicians say to people with low back pain. The Annals of Family Medicine. 2013 Nov 1;11(6):527-3
 We could perhaps determine this interaction between layers as the wider impact OF the problem rather than just as impacting ON the problem. Rather than seeing the BPS as a direct treatment model where we dissect the three domains to find new pain ‘drivers’ to treat, the BPS perspective should really be seen as a CLINICAL philosophy and guide that can be used for improved patient care.Here is another interpretation from a recent paper
We could perhaps determine this interaction between layers as the wider impact OF the problem rather than just as impacting ON the problem. Rather than seeing the BPS as a direct treatment model where we dissect the three domains to find new pain ‘drivers’ to treat, the BPS perspective should really be seen as a CLINICAL philosophy and guide that can be used for improved patient care.Here is another interpretation from a recent paper 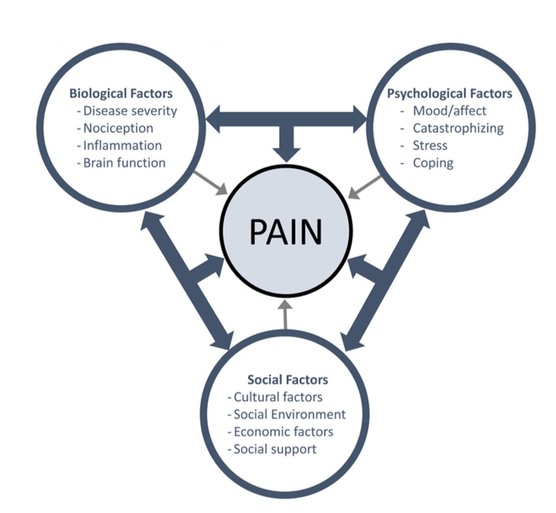 (Figure Fillingim 2017)
(Figure Fillingim 2017)