“The tricky part is that concussion signs and symptoms are not always straightforward and the effects and severity of injury and safe return-to-play can be difficult to determine”
– Mark Lovell
“That’s kind o the line I’ve got to walk now. I think the difference is the post-concussion is light-headedness, where I get that disconnect. Anything else is working and getting your heart rate up. I’m still a little nervous. It’s still a little scary”
– Keith Primeau
The sound from the hit echoed through the arena.
He laid there motionless on the ice.
The other players stared at us with a look of disbelief on their face.
As we opened the door to the bench to step on the ice, two players grabbed me and the AT to help get us to their team mate.
We crouched down beside him trying to get as good of an assessment as possible.
Thank god…he’s breathing.
Getting as close as I could to him to speak, to block out what was happening around us I simply asked “are you there?”.
He responded “yeah my head hurts, I just got my bell rung”.
“Can you move your legs?” Glancing down, they moved.
“Does it hurt if you try to move your neck?”
“No, it’s good, just my head”
As we stood him up and took him back to the bench, it was immediately noticeable, he wasn’t acting like himself.
Once in the treatment room, we could set up for a better more thorough assessment.
He was groggy and lathargic. He lost his usual jovial attitude.
Everything bothered him and his headache was getting worse.
Even the lights in the room were causing an issue.
So was it just a headache? Does he remember what happened? Is there something more going on?
The AT went to work with his assessment. He started asking the player a bunch of questions as I sat back and watched.
Some of the questions made sense.
Do you remember the hit?
Do you know what day it is?
Do you know approximately what time it is?
Then he gave the player a list of words and asked him to repeat it back.
Elbow, apple, carpet, baby, saddle, bubble.
I sat there with a dumb look on my face trying to remember the words too, couldn’t do it.
Afterwards the AT explained what he was doing and showed me this document called SCAT2. I had never seen it before.
First Aid Protocols For Acute Concussion
As research develops so does concussion protocols.
People of my generation probably remember as kids the only thing we were asked was: “how many fingers am I holding up” as if we were Billy Bob on Varsity Blues.
Back then there was talk about “degrees, grades or severity” of concussions, but that thinking is out the window now. There is no such thing as a “minor” concussion anymore.
When I started working in sport the SCAT2 document was the more commonly used method for concussion protocols. It has since evolved into the SCAT3.
Part of the SCAT3 is using the Glasgow Coma Scale (GCS) to assess level of consciousness before you decide to move an injured person. The GCS has been around as an assessment tool for years and if you take advanced levels of First Aid it is incorporated into those courses.
The GCS is used to decide if an injured person requires immediate transport to advanced medical care. It assesses the person on three different types of response (eye, verbal and motor) and gives them a numbered grade according to response. It looks something like this:
Eye Opening
Open Spontaneously (4)
Open To Speech (3)
Open In Response To Pain (2)
Do Not Open (1)
Verbal Response
Communicates Normally (5)
Confused (4)
Inappropriate Words (swearing) (3)
Confused Sounds (groaning etc) (2)
No verbal response (1)
Motor Response
Obeys Commands (6)
Localizes Pain (swats your hand away) (5)
Flexion To Pain (elbow flexes in direction of pain) (4)
Abnormal Flexion To Pain (3)
Extension To Pain (2)
No Response (1)
Once you designate a score for each level of response you add the scores together for a total. If it comes out to less than 15, the person should be transported to hospital for more advanced care due to the possibility of a brain injury. There is a great video you can watch here to see how it is done.
The player in the story above scored a 15, his eyes opened spontaneously, he obeyed movement commands and could communicate just fine so we were okay to take him to the dressing room.
SCAT3 A Valuable Tool For Massage Therapists
Once the GCS is complete and determined it is okay to move someone, the rest of the SCAT3 can be used for assessment.
The document goes through several other assessment tools that include symptom evaluation, cognitive assessment, neck examination, balance and coordination examinations.
This is where those memory techniques of saying five words to the athlete and having them repeat the words back is completed to get an idea of their cognitive function.
Symptom evaluation is assessed by noting things like headaches, pressure in the head, sensitivities to light and noise along with feelings of anxiousness and sadness. Few things are tougher than watching a young athlete cry uncontrollably because of a head injury and being frustrated by not being able to understand what’s going on.
The SCAT3 also goes through return to play protocols for athletes. Most importantly is that once an athlete (or anyone for that matter) has been diagnosed with or assessed a concussion, they must be referred to a doctor (preferably a sport med doctor) to receive clearance to start physical activity again.
Typically with a sports team each player is evaluated on the SCAT3 at the start of the season. This gives training staff a baseline to compare in case someone sustains a head injury. If the original is kept on file, it can then be used as a comparison during the acute injury and also as part of the return to play.
While this document was intended for athletes, it could be a valuable tool to be used in a clinical setting with anyone who comes in that has suffered a head injury whether in the workplace, MVI, or as the result of a fall.
Making the SCAT3 part of your intake, combined with regular communication with the patients doctor could give you a better idea how the patient is progressing.
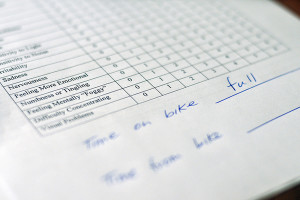
Photo by: University of the Fraser Valley
Massage Therapy Treatment For Concussions
Most people dealing with Post Concussion Syndrome will experience a variety of symptoms ranging from dizziness to headaches and balance issues as well as depression.
In order to help any patient that comes to you who has suffered a concussion, one of the biggest things we need to understand is the Mechanism of Injury that caused the concussion.
Was it a car accident?
Sports injury?
A fall?
Has the person suffered a concussion before?
Which direction did impact come from?
Most concussion treatment revolve around aerobic exercise (after periods of complete physical and mental rest) and then return to play protocols for athletes working up to full contact practices (depending on which sport).
When a patient suffers an injury significant enough to cause a concussion it is likely that they have also suffered an injury to the neck which can contribute to headaches as well as dizziness. It is important for us to try and differentiate where the patients dizziness is coming to discern if it is cervicogenic dizziness or a vestibular issue.
I asked a sportmed doctor why they always refer their concussion patients to a Massage Therapist and he said “it’s because there is usually a whiplash injury associated with the concussion, so getting treatment for anything associated with the neck helps in the concussion treatment”. One study showed that Massage Therapy helped a 23 year old athlete by having two 45minute treatments focused around the pelvic girdle, neck and atlanto-occipital and atlanto-axial joints one month after injury.
The SCAT3 (or any other acute concussion assessment tool) is important for Massage Therapists to understand because it will give the therapist better insight, not only on what was done to help a person immediately, but also as a tool to see how a patient is progressing. Above all when it comes to treatment, your clinical experience is going to be the best guide on how to treat someone with post concussion syndrome. While these tools were intended for athletes, it can also be a great tool in dealing with MVI and workplace injured people who are referred to you. Quite often these ones will be dealing with issues like depression, lack of focus, irritability and not understand why they feel this way. Using these tools can be a great method of tracking their progress and helping you refine or change your treatments according to their needs. There is always a concern around Second-Impact Syndrome where someone sustains a second head injury before the initial concussion symptoms are gone. There are companies starting to develop new protocols and services to help with concussion management like imPACT, King-Devick Test, Shift and axonsports but these all come with a cost. Using free resources like the SCAT3 and CATTonline are widely recognized and may be more suitable for sideline and clinical settings for you until the others are more affordable. Take it from someone who has suffered major head injuries in the past, this needs to be managed properly for successful outcomes, the delay in recovery can be frustrating and depressing. But hey, at least when it happened to me I thought I was in Hawaii, and my dad said it knocked some sense into me!


